

Introduction:Acute myeloid leukemia (AML) real-world incidence has been investigated in a limited number of European countries such as Sweden, Denmark and a few others. These prospective population-based analyses give a more precise idea of AML as a health problem than registry data from cooperative groups or other sources, that usually include selected cases as part of research studies and/or therapy trials. In October 2016, the Autonomous Government of Catalonia funded a project (PERIS SLT002/16/00433) to prospectively collect all AML cases from our territory.
Objective:To investigate the incidence, characteristics and treatment decisions in all consecutive AML patients diagnosed in Catalonia between January 2017 and December 2019.
Methods:Inclusion criteria were diagnosis of AML according the WHO 2016 criteria, both primary and secondary (APL excluded) with an age >18 years. The project was disseminated to all hospitals from Catalonia regardless of their size, having at least one hematologist. A specific informatics tool was implemented for remote reporting of the cases. All data were anonymized. In parallel, a circuit for centralized bio banking of patients' samples was designed. The database included the main clinical, laboratory data as well as the initial therapeutic approach. Cases included in our CETLAM group cooperative studies were automatically linked to the trial database for collecting detailed information. Statistical analyses were performed with R packages.
Results:Assuming an incidence of AML of 4 cases per 100,000 inhabitants (based on previous reported data from others), we expected 912 cases during three years in the 7,6 million population of Catalonia. Our prospective registry included 750 consecutive AML patients, 82% of the expected cases. The remaining 18% could be explained by the exclusion of APL, age below 18 years, or underreporting. Seventy percent of patients (n=527) were diagnosed and treated in the 5 large University Hospitals from Barcelona and the two adjacent cities (Badalona and Hospitalet).
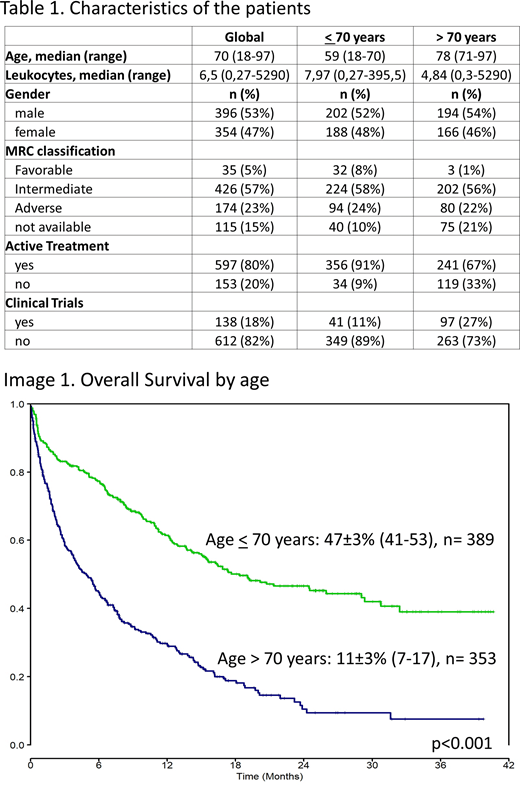
Table 1 shows the main characteristics of the patients. Among the 390 patients up to 70 years, 272 (70%) were enrolled in the CETLAM AML-12 protocol that included intensive chemotherapy (ICT) and risk adapted hematopoietic cell transplantation (HCT). Forty-one additional patients (11%) in this age group received other ICT in different clinical trials. A remaining 73 patients (20%) were treated with other intensive or non-intensive approaches outside trials.
In the group of 360 patients older than 70 years only a 33% (n= 119) were treated under the risk-adapted CETLAM AML-16 protocol for elderly AML patients. This trial included ICT as in the CETLAM-12 in case of favorable genetic features; this was received by 13 of the 119 patients (11%) enrolled. The remaining patients of CETLAM-16 were treated with low-intensity chemotherapy (oral fludarabine, subcutaneous (SC) cytarabine and G-CSF or azacytidine) and 97 additional elderly patients were included in other clinical trials mostly with targeted and hypomethylating agents (27%). Other active therapies outside trials (usually low-intensity) were administered in 50 additional patients (14%) whereas the remaining 94 patients (26%) only received supportive measures (transfusions, hydroxyurea, antibiotics, palliation, or no treatment), because of one or more of the following: advanced age, poor AML features or severe clinical condition.
Overall survival (OS) of the whole series at 2 years was 31±2% (CI: 27-35). Patients younger than 70 years had a 2-year OS of 47±3% (CI: 41-53) compared to 11±3% (CI: 7-17) for those above 70 years (p<0.001) (Image 1).
Conclusions:This prospective study is highly representative of the diagnosis and treatment of AML in Catalonia. The median age at diagnosis was 70 years. Of note, 81% of patients up to 70 years were enrolled in ICT trials. The proportion of patients in trials in the elderly group was lower although still remarkable (60%). In this advanced age group, a 26% of patients were treated with supportive measures only. Despite the high inclusion rate in clinical trials, only one third of newly diagnosed AML patients have the probability to survive at 2 years, with a dismal outcome in those above 70 years. Therefore, the investigation of novel and more effective treatments remains mandatory. This series will be detailed and updated during the meeting.
Salamero:Pfizer:Consultancy;Jazz Pharmaceuticals:Consultancy, Honoraria;Daichii Sankyo:Honoraria;Novartis:Consultancy, Honoraria;Celgene:Consultancy, Honoraria.Olivera:BAYER:Consultancy;Pfizer:Consultancy, Speakers Bureau;Daiichi Sankyo:Consultancy, Speakers Bureau;Boehringer Ingelheim:Consultancy, Speakers Bureau.Sureda Balari:Celgene:Consultancy, Honoraria;Merck Sharpe and Dohme:Consultancy, Honoraria, Speakers Bureau;Sanofi:Consultancy, Honoraria;Novartis:Consultancy, Honoraria;Gilead/Kite:Consultancy, Honoraria;Janssen:Consultancy, Honoraria;Incyte:Consultancy;Roche:Honoraria;BMS:Speakers Bureau;Celgene/Bristol-Myers Squibb:Consultancy, Honoraria;Takeda:Consultancy, Honoraria, Speakers Bureau.Ribera:Pfizer, Amgen:Research Funding;Pfizer, Amgen, Ariad, Novartis:Consultancy, Speakers Bureau.Sierra:Jazz Pharmaceuticals:Research Funding;Pfizer:Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau;Daiichi Sankyo:Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau;Abbvie:Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau;Novartis:Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau;Astellas:Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees;Roche:Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees;Gilead-Kite:Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal